On August 7, the Trump administration quietly pulled the plug on a program that protected immigrants from deportation while they or their relatives received lifesaving medical treatment in the US. Since then, it has partially backtracked the change after being widely criticized, but the future of the medical deferred action program remains uncertain.
For immigrants like Maria Isabel Bueso, who came to the US from Guatemala when she was seven years old at the invitation of American physicians, elimination of the program would essentially be a death sentence. Bueso has mucopolysaccharidosis VI, a genetic disease so rare that clinical trials for treatment struggle to find participants. Bueso, now 24, has been treated for the disease at the UCSF Benioff Children’s Hospital in Oakland, California, since 2003.
“The breakthrough that came from the trial has helped people with the disease live longer than 30 years,” report Miriam Jordan and Caitlin Dickerson for the New York Times. “Before the drug, they rarely survived past 20.”
The policy change is the administration’s latest tactic to harm immigrant families. It comes on the heels of a final public charge rule that creates more hurdles for impoverished immigrants, the forced separation of immigrant children from their parents at the US-Mexico border, and the detention of immigrant children in facilities that one pediatrician said “could be compared to torture facilities.”
Immigrants Receiving Lifesaving Care Put at Risk
The United States Citizenship and Immigration Services (USCIS) is part of the Department of Homeland Security (DHS), which processes applications for family immigration and citizenship. Until last month, USCIS allowed immigrants and their relatives undergoing lifesaving treatment to stay in the US for two-year periods until they were fully treated. The agency receives about 1,000 deferred action applications related to medical issues each year, Jordan and Dickerson report.
Without a public announcement or public comment period, USCIS field offices began sending denial letters (PDF) to deferred action program participants like Bueso. “You are not authorized to remain in the United States,” the letter reads. “If you fail to depart the United States within 33 days of the date of this letter, USCIS may issue you a Notice to Appear and commence removal proceedings against you with the immigration court.”
What the policy change “means in practice is that noncitizens — some of them children — may lose access to their health care,” the Boston Globe Editorial Board writes. “Forcing patients to leave the United States and its health system amounts to a virtual death sentence if patients’ home countries can’t handle the complex medical needs that brought them here in the first place.”
Indeed, if Bueso were deported to Guatemala, she would not be able to receive the treatment or medical care that has allowed her to graduate summa cum laude from California State University, East Bay; intern in California Assemblymember Rob Bonta’s office; and advocate nationally for people with rare diseases.
Bueso was receiving her weekly treatment at UCSF when she learned that she could be deported, KQED’s Farida Jhabvala Romero reports. “My mom and I, we started crying together. I started shaking,” said Bueso. “It was just a shock for me, because I depend on that treatment.”
DHS Calls an Audible
As part of the policy change, DHS shifted responsibility for handling medical requests for deferred action from USCIS to a sister agency, US Immigration and Customs Enforcement (ICE), which makes arrests and supervises deportation. But ICE has been blindsided by the lack of transparency around the elimination of the program. “An ICE official said that the department had not been notified in advance about the change and questioned the agency’s ability to assume that role,” Jordan and Dickerson report.
The policy change did not gain traction until the end of August, and the administration was immediately hammered by public outrage. More than 120 members of Congress sent a letter of concern (PDF) to top officials at the Department of Homeland Security, Shannon Dooling of WBUR News reports. “We urge you to immediately reverse this shift in policy, resume consideration of these urgent requests, provide the justification for the policy change, and provide clarification on the agency’s plans for implementation,” the lawmakers wrote on August 30.
“This is a new low,” Senator Ed Markey (D-Massachusetts), one of the letter’s coauthors, told the Associated Press, “Donald Trump is literally deporting kids with cancer.”
Faced with criticism, USCIS partially backtracked its policy change over the Labor Day weekend, announcing that it would reopen all medical deferred action cases that were pending on August 7. However, the agency did not clarify whether it would continue the deferral program after processing the current applications, Miriam Jordan writes in the New York Times.
The USCIS decision buys Bueso some more time in California. “It appears that the administration is revising its new policy, and we are hopeful that it will grant an extension of Isabel and her family’s medical deferred action status,” Bueso’s attorney, Martin Lawler, said in an email to KTVU. But nothing is certain for her or other immigrants in a similar situation.
Bueso is scheduled to testify on September 11 at an emergency hearing on the policy change at the House Committee on Oversight and Reform. You can watch it here.
The post Deadly Policy Change Blindsides Immigrants with Severe Illnesses appeared first on California Health Care Foundation.








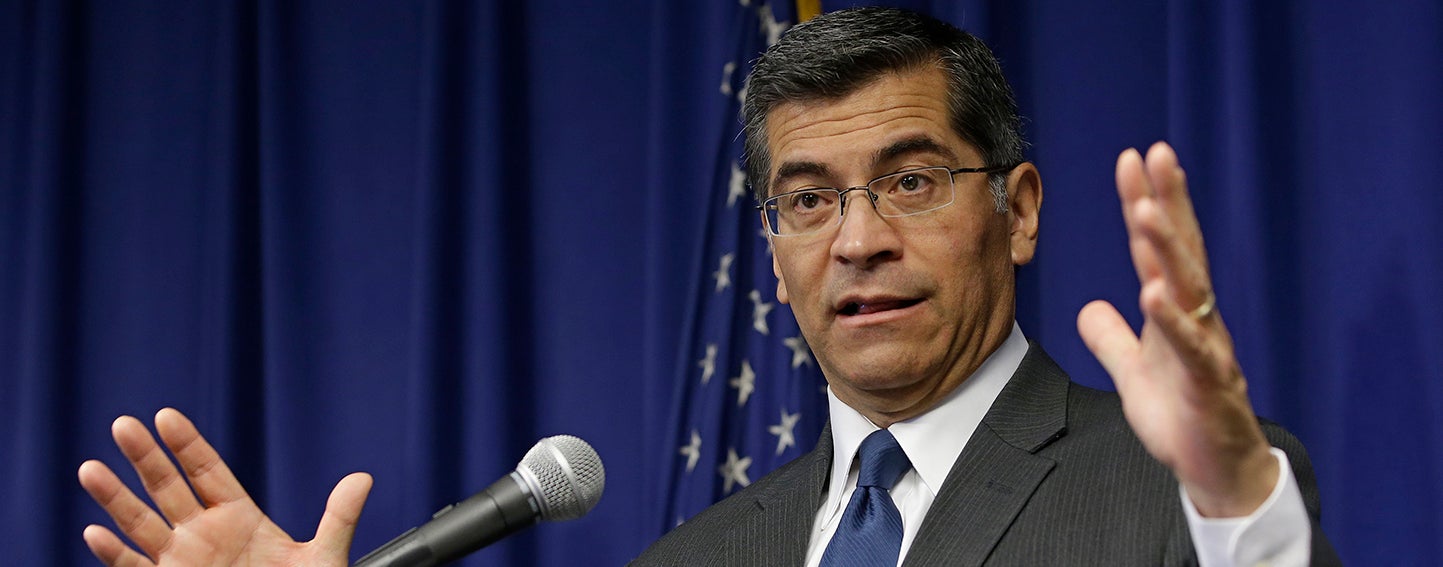 California Attorney General Xavier Becerra alleges that Sutter Health used its pre-eminent market power to artificially inflate prices. Photo: Rich Pedroncelli/Associated Press
California Attorney General Xavier Becerra alleges that Sutter Health used its pre-eminent market power to artificially inflate prices. Photo: Rich Pedroncelli/Associated Press